

This World Mental Health Month, we reflect on what healing takes in the face of war trauma and genocide. Since the founding of Healing for Gaza in July 2024, we have grown from a team of three to 150, offering over 1600 psychotherapy sessions and group work for children, adolescents, parents, and frontline workers.
In this blog, we interview two war trauma psychotherapists and psychologists, Justine Hardy and Dr. Alexandra Chen, who bring a combined almost 50 years of experience working with children and adults affected by extreme violence and genocide. Together, they train, supervise, and lead clinicians at Healing for Gaza and lead the design of our clinical model.

Justine is a trauma psychotherapist and former journalist who has worked with refugees from Bosnia, Afghanistan, the Kashmir Valley, Pakistan, Yemen, Syria, and other countries for over 30 years. In 2008, she founded Healing Minds Foundation, a mental health charity based in Srinagar, Kashmir’s summer capital. In addition to her clinical work, she serves as senior clinician, trainer, clinical supervisor, and lead facilitator of individual and group breathwork at Healing for Gaza.

Alexandra is a trauma psychologist who has worked with war-affected children and their families in the Middle East and Africa for the past 17 years. She founded Healing for Gaza in 2024 and currently serves as our Executive Director, responsible for designing our clinical model, training clinicians and interpreters, and offering expertise on trauma therapy for children, parents and male victims of torture.
In this blog, Justine and Alexandra share ten key lessons learned over the past 14 months. These learnings have guided our team in offering quality clinical mental health care for hundreds of Palestinians from Gaza.
1. Self-Regulation First
Our patients endure experiences that no human should ever have to face. The scale of violence, dehumanisation, instability, and bloodshed witnessed during Israel’s genocide in Gaza has inflicted layers of war trauma on over two million Palestinians from Gaza. Our clinicians thus listen to heavy and dark stories of grief and loss weekly, and witness a level of suffering that can be difficult to process, even for seasoned mental health professionals. In order for therapists to hold space for our patients to heal from their traumas, they must be continually attuned to their own emotional state in order to stay grounded as a foundation for the healing work.

Justine and Alexandra facilitate a breathwork exercise during a clinician self-regulation training session.
Justine: Therapists learn to adopt a particular posture of listening, to make sure their patient knows they’re with them and paying attention. But what you hear will constantly push questions in your mind about your own beliefs about what you care about and what you think is important. So as you listen, an internal narrative is spinning, so you cannot drift off. One of the maladaptations that therapists can experience is falling into the trap of thinking about what they want to say, rather than giving their full attention to what they are being told. These are situations and stories that need absolute focus and attention — absolute presence.
Alexandra: Just the act of being present is challenging — to be fully present with the depths of your patient’s pain. On one hand, it is only natural to be dysregulated in that moment — to feel one’s stress responses hyperaccelerate, or have an urge to dissociate. On the other hand, our role as clinicians in the face of war trauma requires us to have a heightened level of emotional capacity and self-awareness. Thus, a core part of our War Trauma Curriculum is helping each clinician (1) identify how our own nervous systems are reacting to this level of suffering; (2) learn what we need to be able to do to ground ourselves and remain present; (3) become aware of where our individual boundaries are; and (4) figure out also how to lean upon one another in supervision and as a cohort. Ultimately, this work requires us to do this together.
2. Assume Less
On average, HFG clinicians bring 16 years of clinical experience as psychotherapists, psychologists, and psychiatrists. Yet for the vast majority of our team, this is their first time working with people affected by an active genocide. But in this unique context, what assumptions do we have to let go of in order to provide therapy appropriately?

Justine and Alexandra speaking on a panel on war trauma at HFG’s first World Children’s Day celebration in London, Nov 2024
Alexandra: There is fundamental unlearning that needs to be done among all of us who have been trained in more classic models of trauma therapy. One of the first things we say to our clinicians is: “Each session could be your last.” Reconciling this reality alone can be quite shocking for those trained in modalities that assume at least a dozen sessions. So, the question is simply, what can you do today?
Justine: Our therapists are used to working with people who are moving in and out of their sympathetic nervous system [the body’s alarm system that is activated with heightened emotions]. Patients will be in a distressed state at times, but they will have the opportunity to come out of it. What a lot of our therapists are finding difficult is that our patients [from Gaza] are in their sympathetic nervous system constantly. You’re not talking about the past; you’re not doing the standard ideas of what therapy is. It’s the immediacy of this moment right now that is happening for this patient, so we must first perform psychological first aid. It’s quite discombobulating and unsettling for them at first, as they’re having to completely reframe the way that they’re working.
Alexandra: We encourage clinicians to be open and courageous to critically challenge what we’ve learned through Western and Global North frameworks that were ultimately designed for different communities, different contexts, and different privileges. For starters, most therapeutic models are based on an assumption of safety. This baseline simply does not apply in the context of Gaza – and has significant implications for what ‘boxes’ are safe enough to open in therapy, what kind of psychological support is needed for survival right now, as well as the level of transference we should expect from our patients in such volatile circumstances.
3. Slow Down
On one hand, the notion of “each session could be your last” can lead clinicians to feel as though everything has to be addressed in one session. Nevertheless, slowing down is powerful. The pace at which our therapy sessions operate requires our clinicians to be more deeply in tune with their patients and mindful of their emotional safety when talking about their trauma.

Alexandra and Justine co-leading polyvagal exercises during a self-care training for staff from NGO partners Ghassan Abu Sitta Children’s Fund and Wings for Hope
Justine: It is human nature to speed up when contending with scenarios as acute as those which our patients are living through. Even very experienced mental health practitioners find it very hard to slow down and find that balance. When somebody is in a very distressed state, you help them by the way you, as the therapist, are breathing…by the way you’re sitting… by the speed with which you’re speaking. Our voices are low and calm, and that is intentional to make patients feel more at ease.
Alexandra: Slowing down both our internal thoughts and external words can not only be an effective strategy for co-regulating a patient’s nervous system, but is also a core part of our ethical practice of not opening more boxes than we can close. Something as simple as inviting a patient to feel their own two feet on the floor can cause one to weep — crying just to feel safe enough to be present in their own bodies for the first time.
Slowing down is also part of our promise to our patients that they do not need to tell us everything at once and that we are committed to being here for them for the long haul. Our steadfastness can help ensure patients do not retraumatise themselves by narrating and reliving too much trauma all at once. Shwaiye shwaiye [“slowly slowly” in Arabic], as we say.
4. Radical Listening
When we as clinicians are able to stay self-regulated, assume less, and slow down, the doors then open to hear and hold the heaviness of what is being shared in therapy. This includes listening for the different cultural ways in which Palestinians may resource themselves, as well as for the indirect ways in which patients describe the impact of war trauma, including marital conflict or disordered eating. Radical listening thus requires our team to push past our own assumptions about how one should express emotions or process their trauma in a genocide.

Alexandra and the children of Gaza learning about all the countries around the world that the HFG team come from
Alexandra: Learning about our patients, what matters to them, and what they need from us requires a whole different level of listening. It entails observing and keeping our minds open for what constitutes strength and fragility in ways that may be unfamiliar or contradictory to our own cultures. For example, when you ask a Palestinian child, “How are you?” and he says “Al7amdilla, ana mni7 (Praise God, I’m well)” but then goes on to share with you how his mum is depressed and can’t get out of bed, his father is crushed because he isn’t allowed to work as a refugee, that his sister just had another miscarriage, and his brother is so angry he’s punching walls… a Western-trained therapist might make the mistake of taking an individualist lens and saying, “Ok, that sounds hard, but tell me, how are YOU?” to which the child will probably respond, “But I just told you how I am….”
Justine: Many adults we speak to also do not want to talk about the war. They come to it in circular and roundabout ways. After experiencing this level of devastation, patients are likely to feel wary of talking about it, both for fear of replaying the agony for themselves and also for fear of the therapists not being able to handle it. So, we need to be able to listen with the understanding that what we may be told will make it impossible to remain calm. Intense rage may be how the person we are working with protects themselves, and this, too, is something we as clinicians need to be able to sit with and work with.
5. When there is no “Post”
The foundation of trauma psychology as a field has long been centred around the concept of PTSD — Post-Traumatic Stress Disorder — a diagnosis first coined in the 1970s and 80s to describe the symptoms of American war veterans experiencing flashbacks and night terrors despite being safely back at home in the United States. Consequently, most trauma research and interventions are designed around PTSD and carry an underlying assumption that the trauma is “post” and that patients now have access to safety. How, then, can clinicians best support trauma healing when there is no ‘post’?
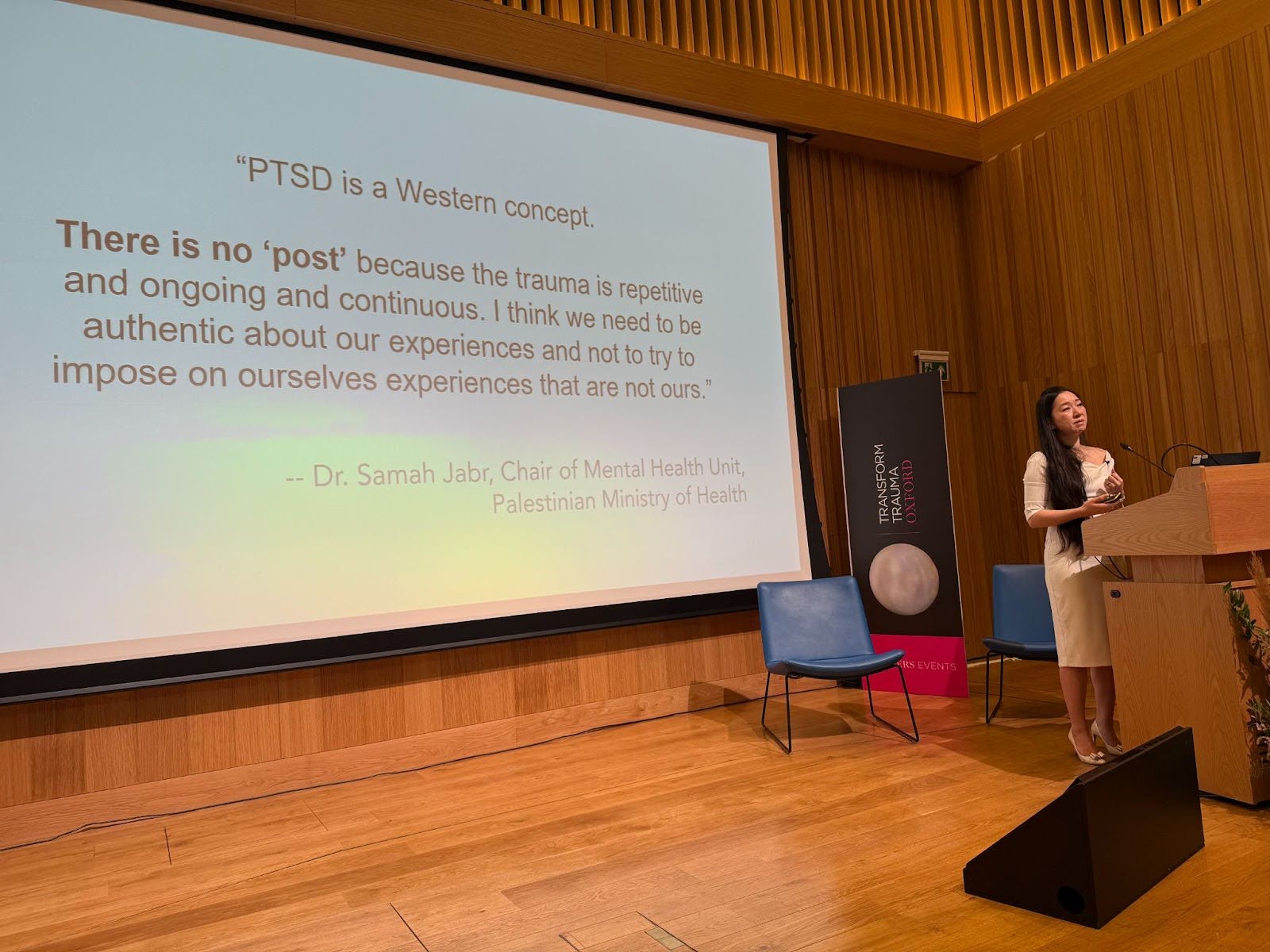
Alexandra’s individual talk on war trauma at the Oxford Trauma Conference, Sep 2025
Alexandra: So much of our work as a team is an intentional commitment to unlearning that which is irrelevant for contexts of war, and learning new ways that are resonant. For example, in contexts where patients have access to safety, trauma responses such as hypervigilance and dissociation are typically viewed as symptoms to be regulated. However, in contexts where threat and deprivation are ongoing, these same responses are often vital for survival. As clinicians, our job is, then, to identify their adaptive role in helping our patients survive — instead of trying to uniformly down-regulate them (and in doing so put our patients’ lives at risk), for us to find ways to help them breathe when they need to sleep, or to scale back from a mounting panic attack.
Justine: In the context of violence this extreme, people may need to hold onto aspects of what could be termed as “dysregulation.” In the case of our Palestinian patients from Gaza, it may well be that their rage and anger are protecting them, and may be the key to their immediate survival. Anger and rage are so often the human cover for fear. They can be vital armour.
Alexandra: Especially in an ancient culture of shame and honour, rage is often the only energy that feels dignified and prevents a patient from collapsing. For those familiar with Arabic, in a lot of ways, sacred rage as therapist Linda Thai calls it is the other side of qaher [an Arabic term with no direct equivalent in English, describing a deep-seated feeling of anger and helplessness caused by prolonged, inherited injustice] — as it is the only way for the volume of one’s qaher and anguish at injustice not to crush the spirit.
So you can imagine if a therapist were to try to quickly calm or minimise this rage — this not only can make them feel unheard, but may also harm their abilities to survive.
6. Bear Witness, do not “Fix”
Although the genocide is affecting hundreds of thousands of Palestinians, many feel isolated and abandoned. Being able to share their feelings without judgment or pity can offer meaningful relief and ease some psychological burdens. For many of our patients, therapy is one of the few places where they can just let it all out. It is important that when they express their feelings, they feel held by professionals who can hold and handle the heaviness and darkness. To accompany someone as they navigate what has happened to them is to bear witness.

Justine leading an interoception exercise to calm the nervous system with HFG clinicians and interpreters
Justine: Clinicians may find it hard not to try and offer solutions to what they are being told, because being present becomes so hard. It is this bearing witness that may be what is needed more than anything else. In a sense, the clue is the word ‘bear,’ to be able to be steady, to ‘bear’ the weight of what has happened to them without shying away from it.
Alexandra: Healing is not fully possible until you’ve had an opportunity to properly grieve. And more often than not, our instinct is to move past the pain because it’s painful for us to hold. Yet holding space for validating the profound grief is critical as a first step for healing.
I’ll explain what I mean more fully in the words of a 26-year-old patient in Gaza, who sounded twice her age when I first spoke with her, her voice having aged with the weight of her burdens. She cares for four children — two of her own and two of her martyred sister’s. Her husband had also been martyred a month prior. She was the sole person responsible for her elderly parents, one of whom suffers from dementia. Remarkably, she said, “I have surrendered to the fact that we might not make it. That if this is what God has written for me, I accept.” When I asked her why she even came to therapy, and what she wanted from us, she said, “I know that this is a test. First, help me succeed in this test: to not lose my faith as I watch all four children starve — to not give up. Second, if nothing else, then at least someone will have witnessed my life, will know all that I have endured and sacrificed, and that I was brave, because I cannot share these things with the people closest to me.” The notion of bearing witness is much larger in a context of erasure.
7. Options and Agency
One of the main tenets of the Healing for Gaza model is to interact with our patients with respect, dignity, and offer patients choice wherever possible. HFG currently offers sessions both in person and online; video or voice-only; internet or phone-only. During the initial triage, patients can choose whether they’d like to work with a native Arabic-speaking clinician or with an English-speaking clinician with an interpreter, as well as make requests for religious or other identities.
On the clinical front, HFG is flexible with patients and their needs. Patients are empowered to choose the path of healing that feels most right for them – individual or group sessions, talk therapy, breath/bodywork, and or expressive therapies are all available.

Alexandra and Justine co-training NGO partner staff from GEMS and HEAL Palestine on the neuroscience of trauma and the vagus nerve
Alexandra: Sometimes, a patient isn’t ready to speak about their suffering but just needs breathwork to help them calm their nervous system enough to make an important decision, and that’s perfectly ok.. On the technology side, we also try to offer agency. For example, one of my patients had bad internet one day and couldn’t turn on her camera in the session, so we just relied on audio. She disclosed quite a few deeply traumatic things with me that day, and later revealed that she opened up because she felt more comfortable without her camera on, as she didn’t want to see her own face in so much pain. For our group in-person work, sometimes the volunteers that help me keep the children focused – however I am less interested in them being ‘obedient’, and more interested in them feeling free. If what we offer resonates for them that day, they will stay, or wander back after a little run around in the garden outside, and how wonderful is it that they might feel safe enough with us to do that?
Justine: As Alexandra puts it, offering choice is a way of supporting those who feel wholly dehumanised. One of the most repeated phrases we hear is something along the lines of, “I had no choice.” Whether we are working with those still in Gaza or those displaced, almost all choice has been removed, either by the direct violence or by having little or no rights once they have left. The offering of choice, and the chance to have agency, can for some feel a first small step towards reclaiming themselves.
8. Patience
Patience is essential for providing meaningful and compassionate mental health care. On the technological front, most of our patients are in Gaza and other places in the Middle East where internet access is far slower than what clinicians based in the UK, USA, Canada, or Australia are accustomed to. In addition to connectivity, patients often struggle to find a quiet place to talk, and family members may interrupt a conversation. Additionally, language can slow down sessions, as therapy is often offered through interpreters. Thus, developing a new level of patience is a prerequisite for this work.

Justine leading a breathwork exercise with NGO partner staff from Humanities Without Conditions
Alexandra: At HFG, we ask our clinicians to block 90 minutes in their calendar for each session, even if the actual therapy session is only 50-60 minutes. This is because it may take a patient 20 minutes just to connect, and we want to ensure they still receive the full hour. There’s often a lot of “Can you hear me?” and troubleshooting that needs to happen, but we’re all in it together just to say “we’re here with you”.
Patience and self-compassion as therapists is also important, albeit often difficult. Beyond technology, unlearning the instinct to intervene or address our patients in the traditional ways we were trained to do is also not easy. Offering therapy with an interpreter is also a different learning curve. All these pieces require an unprecedented level of patience and gentleness with ourselves, to ensure that any frustration does not project into the therapy or the patient.
Justine: ‘Can you hear me?’ crackle, crackle. ‘Yes.’ crackle crackle. ‘I can’t hear you.’ crackle, crackle. And on it goes… These scenarios will test anyone, particularly when everyone is already under so much stress. It still amazes me that the Palestinians do not give up on the call when the line breaks down, yet again. Their persistence guides our patience. It can be the same when their children jump into the call, grabbing the phone from their parents. If we can go along with this, engage with the child and the parent together, and make it all fit into the conversation, it can make it easier for the exhausted parent. Particularly when interpreter and therapist, parent and child, are all in the conversation together, in a small therapeutic community.
9. Unexpected Forms of Resilience
An important part of trauma work is a psychotherapist’s responsibility to understand our patients’ values and realities with depth and nuance. In the face of relentless dehumanisation, erasure, powerlessness, helplessness, and humiliation, the Palestinian people continue to embody extraordinary dignity, resilience, and pride, and reclaiming memory and culture have been a central part of trauma healing. Cultural sensitivity will allow clinicians to identify these cornerstones on which they can build foundations of healing, even for patients in exile.

Alexandra, Justine, with HFG Clinicians, Interpreters, and the beautiful and brave women of Gaza
Justine: There are some people who seem to believe that every Palestinian is a member of Hamas. Others who assume that they will be dishevelled and dirty and ragged in their starvation. There are so many assumptions, but what is so often missed is the strength of the sentiment, ‘We will not be broken. We will survive.’ They believe it, and they wear it, arriving beautifully dressed in person, or on calls, even while they are living crammed into tents. If some of those with assumptions were to have a conversation with a Palestinian, I think they would come away amazed by the nuance, even in the face of such devastation.
Alexandra: I have had the privilege of working with Palestinian children and their families for almost two decades, and I still experience awe and humbling encounters with them daily. As an example, Palestinians from Gaza have some of the most exceptional grasp of the Arabic language. They are successful poets, writers, and scholars. And so for many of our patients, children and adults alike, writing and reciting poetry has been an unexpected source of healing, a way to say “I have survived. I am a witness to my people. I am still here!”
Justine: When there’s a sense that people are being made extinct, cultural roots become so vital. It’s the one thing you have left.
Alexandra: Exactly. One of our 10-year-old girl patients showed up to therapy one day, determined to teach me all the Gaza slang – both because she was anxious that she would forget them because of how trauma had been affecting her memory, but also because she wanted to show me her pride in her people. Similarly, the kids learning the Palestinian traditional dance, dabke, during our field missions is a significant moment of resilience. The indigenous tribes of the Native Americans and First Nations have taught this repeatedly: reclaiming culture is essential to healing; preserving and celebrating one’s heritage is resistance to erasure.
10. The end of a war does not mean an end to trauma
It can be easy to assume that once a war has ended, the trauma has ended. That notion is false. The trauma of genocide will take years to heal, and its impact will be passed down generation to generation, and even with therapy, some scars will never fade. People may have healed but not forgotten, making trauma visible in future generations. In many ways, the real healing starts now.
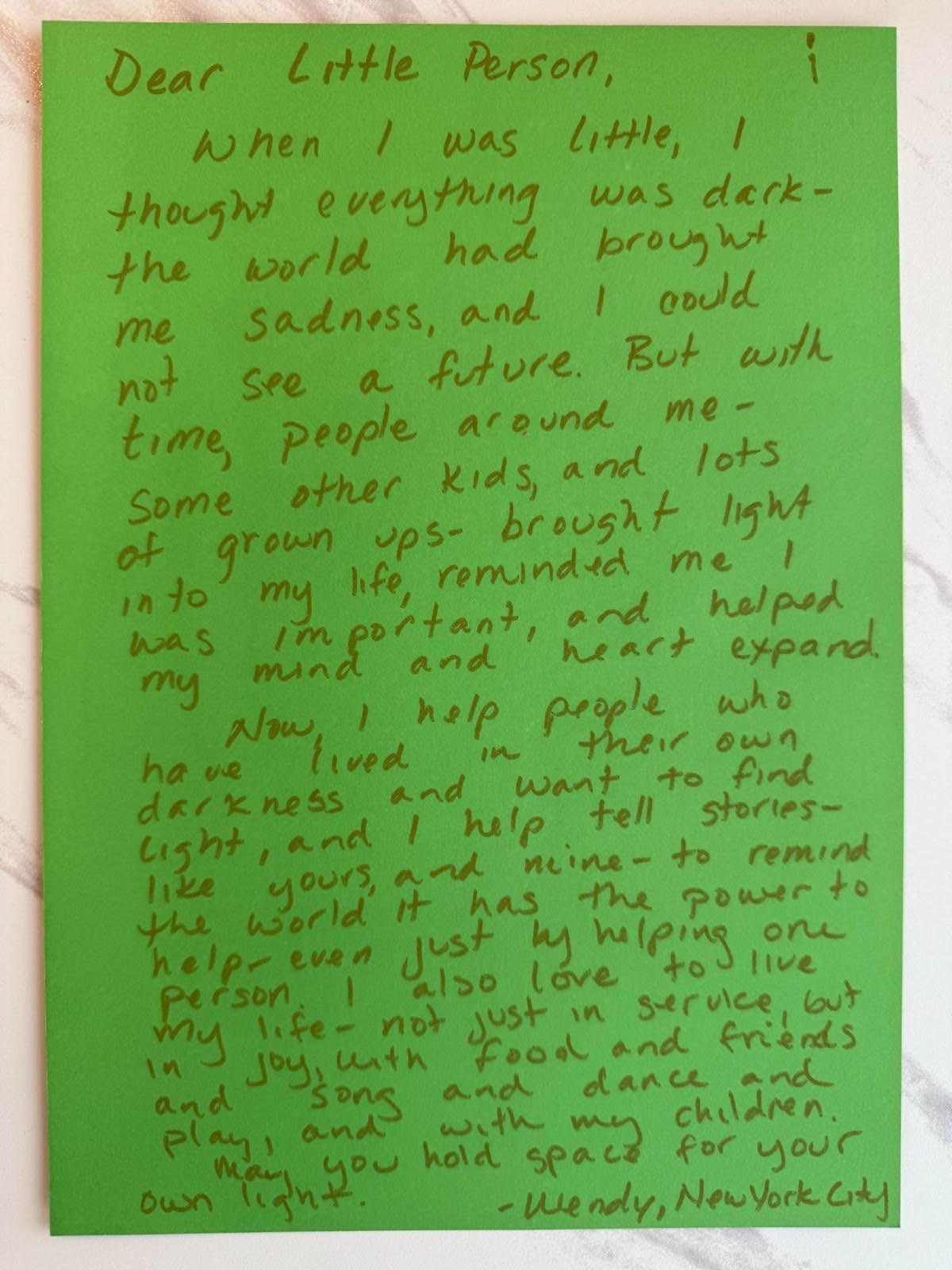
Letters to the Children of Gaza, written by participants at the Oxford conference — here, generational wisdom and hope from a kind human who once knew childhood trauma
Justine: When I first experienced war, more than 30 years ago, I wanted to understand what enabled people to survive and how best that survival could be supported. I founded Healing Minds Foundation* in Kashmir when it was already becoming a forgotten war. Over the three decades and more since, the state of conflict has moved from acute to chronic, but the human damage runs right through, one generation’s trauma moving through into the next.
Alexandra: For me, Justine’s pioneering work over several decades is a model of what can and should be in meaningful trauma work. The suffering that we are tending to with the gentlest of care now is one of the consequences of intergenerational trauma in our world, and that is not lost on us… so the lens of this work not only has to be a lot longer, but also a lot deeper in order to heal.
Justine: Most conflict trauma programs are very much the “move in, move out quickly” option, and in so much of this kind of work, humanitarians or healers are helicoptered or parachuted in. I wanted to create something that was staying in the same place, working with the same people, going deep, deep within the communities. And because we’ve been staying and doing the same thing in the same place for so long, it means that a lot of people have come to work with us and train with us over the years. And that is very similar to what Alexandra’s created with Healing for Gaza.
Alexandra: We are here for the long haul. Thus, the persistent question in the back of my mind as our humble effort evolves is how do we build to last? How do we ensure we can be here meaningfully for our patients, and not abandon them halfway? Ultimately, our healing work is not just individual, not just collective, but the envisioned impact of healing is generational, inshallah. The children deserve better, and our commitment is to keep learning how to do this work better and evolving our model to meet them where they need us most, because it is the least we owe them.
*Healing Minds Foundation is an integrated mental health model combining clinical and holistic practices, psychology, sociology, anthropology, philosophy, and somatic therapy systems, operating from centers in the Kashmir Valley in North India.
As Healing for Gaza continues to provide trauma therapy, the lessons we have learned underscore that mental health care in war settings is constantly changing. We learn every day from our patients and our colleagues to remain committed to adapting, learning, and showing up with compassion for those too often forgotten.
_____

Heidi Ho is pursuing degrees in public health and journalism at Northeastern University. She is driven by a passion for social justice, health, and science. She previously worked with a non-profit organization in Ecuador and currently writes for multiple publications. Heidi currently serves as a communications intern with Healing for Gaza.

Laura Albast, HFG’s Communications and Social Media Coordinator, contributed editorial work to parts of this interview. Laura is a Palestinian journalist, photographer, and media analyst. A professional Arabic-English translator, Laura has also joined Healing for Gaza’s medical interpreter cohort.